



Basal cell carcinoma (BCC) is the most common skin cancer , with about 85% of cases occurring in sun-exposed areas such as the head and neck. However, BCC in the vulva (female external genitalia) is very rare, accounting for less than 0.4% of all BCC cases and only 2–5% of vulvar malignancies.
Patients with vulvar BCC are often white and older women (average age about 70 years). Because this area is not directly exposed to sunlight, other factors such as immunosuppression, chronic irritation, pelvic radiation therapy, or repeated skin trauma can contribute to its development.
In this article, we present a full translation of a case report by Dr. Reza Moeini and colleagues in which a 77-year-old woman with a BCC lesion of the vulva was successfully treated with Slow-Mohs micrographic surgery. The original version of the article was published in the journal Clinical Case Reports
and can be read at this link: Read the full article on Wiley 
Case Report (Case Presentation)
A 77-year-old, multiparous woman presented with discomfort and itching in the vulvar area. She had a pink lesion that had started 2 years earlier and had gradually progressed (Figure 1). The patient had been treated with corticosteroids and antifungal creams, but without success.
In the patient’s history:
Regular medication use, substance abuse, sexually transmitted diseases, smoking, immunosuppression, or any specific disorder were denied.
The patient also denied any personal or family history of skin cancers or internal malignancies.

Figure 1 — Erosive plaque on the right labia majora in a 77-year-old woman in favor of basal cell carcinoma:
(A) at admission, (B) after Mohs surgery, (C) after 13 months of follow-up
On physical examination, a 10 × 4 cm erosive plaque with well-defined borders was observed on the right labia majora. There were no palpable lymph nodes in the inguinal and femoral regions. A complete skin examination also revealed no suspicious lesions. Ultrasound also did not report abnormal inguinal lymph nodes.
To confirm the diagnosis, an incisional biopsy of the lesion was performed. Pathology of the lesion showed:
Neoplastic proliferation of the dermis from small epithelial cells
High nuclear to cytoplasm ratio
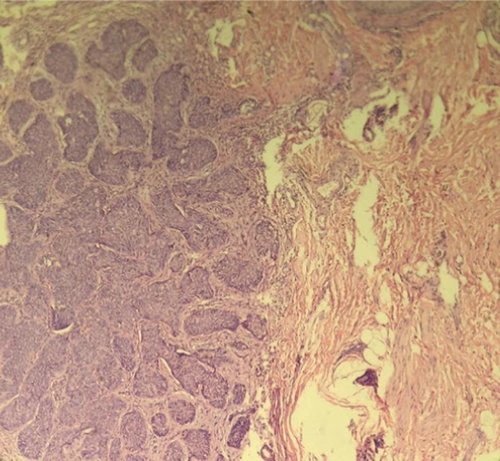
Formation of irregular clusters with palisading of cells in the periphery (Figure 2)
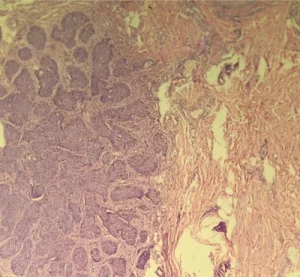
Figure 2 — Histological section showing neoplastic proliferation of small epithelial cells with a high nuclear-to-cytoplasmic ratio and peripheral palisading, in favor of BCC.
The diagnosis of nodular basal cell carcinoma (Nodular BCC) was confirmed and the patient underwent Slow-Mohs micrographic surgery (MMS). At 13-month follow-up, the area had completely healed and there was no evidence of recurrence (Figure 1).
Description
Due to its rarity, vulvar basal cell carcinoma (BCC) has been studied and reported only sparingly. Etiological factors include those implicated in cutaneous BCC, including: radiation therapy, exposure to tar or arsenic, burns, traumatic scars, chronic skin irritation, certain types of immunosuppression, and hereditary skin diseases such as xeroderma pigmentosum and nevoid basal cell carcinoma syndrome. It has also been reported in some cases to be associated with Paget’s disease of the vulva and lichen sclerosus. However, no associated risk factors for BCC were found in the present case.
In contrast to the present case, a review of the literature has shown that there is usually a delay of several years between the occurrence of vulvar BCC and the appearance of symptoms (such as burning and itching).
Clinical manifestations of vulvar BCC are nonspecific and include itching, discomfort, bleeding, pain, infiltrative pigmented lesions, and a palpable mass in the vulvar area. In most women, these lesions are located on the nonmucosal surface of the labia majora. Bilateral or multifocal cases are very rare.
Overall, metastasis is rare in vulvar BCC. However, aggressive histologic patterns (morphea form, infiltration, and basosquamous), large primary tumor size (>2 cm), and occasional perineurial spread are common factors in cases of metastatic vulvar BCC. The most common sites of metastasis include inguinal lymph nodes, bone, lung, and skin.
The best way to make a diagnosis is to biopsy the suspicious lesion. Differential diagnoses for vulvar BCC include:
Inflammatory dermatoses such as atopic dermatitis, psoriasis, lichen planus, lichen simplex chronicus,
other vulvar malignancies such as intravaginal neoplasia (VAIN), Paget’s disease of the vulva, squamous cell carcinoma (SCC)
, and benign vulvar tumors such as seborrheic keratosis are flat.
 Treatment
Treatment
Treatment for BCC can be surgical or nonsurgical.
Surgical methods: curettage, cautery, cryosurgery, Mohs micrographic surgery (MMS), and complete surgical excision.
Nonsurgical methods: radiotherapy and systemic chemotherapy.
The most reliable treatment for basal cell carcinoma is surgery. Methods such as curettage, cautery, and cryosurgery have been used for superficial lesions, but patient acceptance of these methods is low. Also, BCC lesions are moderately sensitive to radiotherapy, and systemic chemotherapy is not effective in treating localized BCC.
Wide surgical excision with the goal of achieving histologically sound tissue margins is considered adequate treatment for most cases of vulvar BCC. To prevent local recurrence, surgical planning should include a 5–10 mm margin of apparently sound tissue and depth to the fascia.
Due to incomplete resection, local recurrence of vulvar BCC has been reported to be about 10–20%; therefore, MMS can be considered as a promising treatment for vulvar BCC.
MMS is particularly used to treat recurrent BCC, large BCC, or BCC with an aggressive histological pattern, and in these cases, cure rates of over 97% have been reported. It is also associated with better cosmetic and functional outcomes.
In the present case, we used MMS to treat vulvar BCC, which had favorable cosmetic results. MMS also provided good margin control and prevented recurrence. Therefore, this method can be considered as the treatment of choice for vulvar BCC, especially given the common delay in diagnosis.
Slow-Mohs method
In this method:
First, the tumor is debulked.
Then, 2 mm of the margins are removed at a 45-degree angle.
The tumor is divided into two or more sections, depending on the size, and numbered clockwise.
Each stained section is fixed in formalin and sent for pathological examination as a horizontal section.
The difference between this method and conventional Mohs is that frozen sections are used in the traditional method. The Slow-Mohs method provides more accurate pathological results and therefore leads to better treatment and follow-up than conventional MMS with frozen sections.
Conclusion
Basal cell carcinoma of the vulva is a rare cancer that may be late diagnosed due to nonspecific manifestations. The best treatment is surgery with careful control of the margins, and the Slow-Mohs method can be considered as an effective and standard option in these patients, especially for the prevention of recurrence.
Source:
This case report was published by Dr. Reza Moeini and colleagues. You can read the original version of the article at the following link:
Treatment of vulvar basal cell carcinoma with Slow-Mohs micrographic surgery: A case report (Wiley)

